Every minute, somewhere in sub-Saharan Africa, a child spikes a fever. Their mother walks to a clinic that may have one microscope, no trained microscopist on duty, and a line of 30 patients.
Malaria caused an estimated 263 million cases and 597,000 deaths worldwide in 2023 . More than 94% of those cases and 95% of deaths occurred in Africa, with Nigeria alone shouldering roughly a quarter of the global burden. Children under five bear the worst of it, accounting for three out of four malaria deaths on the continent, according to the WHO data cited in the review.
For 140 years, since French physician Alphonse Laveran first saw Plasmodium parasites in blood in 1880, diagnosis has meant that researchers stained a slide, and peer through a microscope. It worked, but is slow, labor-intensive, and dependent on skills that are scarce where malaria is most common. Between 2017 and 2023, only about 48% of febrile children in sub-Saharan Africa were taken to a trained provider and received a diagnostic test.
That is the gap a new scoping review tackles head-on in npj Digital Medicine . Researchers Fangxu Xing, Shahar Lazarev, and Jonghye Woo systematically mapped out every major diagnostic method, from Giemsa-stained microscopy to loop-mediated isothermal amplification (LAMP), and then traced how artificial intelligence is changing the field.
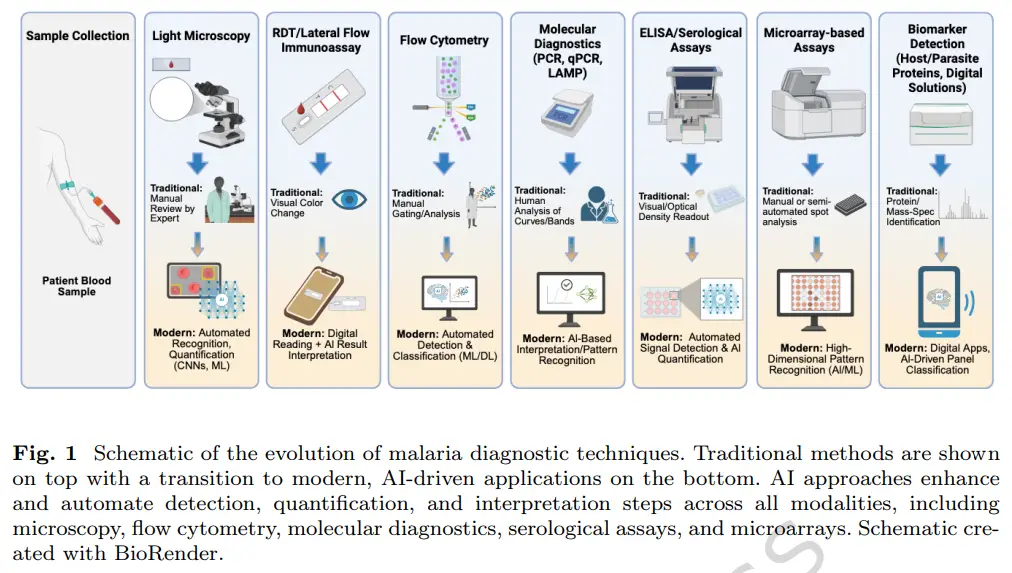
Their conclusion is that AI, especially deep learning models that learn to spot parasites in digital images, is not replacing doctors any time soon, but rather, is acting as a tireless assistant that can deliver expert-level reads in seconds, on a device that fits in a backpack, and in places where experts cannot be stationed full-time.
This post follows their review step by step, translating the technical detail into plain language. We will look at why diagnosis is so hard, what traditional tools can and cannot do, where AI is already outperforming humans in controlled studies, and what still needs to happen before a phone-based test in a rural area is as reliable as a reference lab in Boston.
Why a fast diagnosis changes everything
Before we talk about microscopes and algorithms, it helps to be clear on what we are actually trying to find.
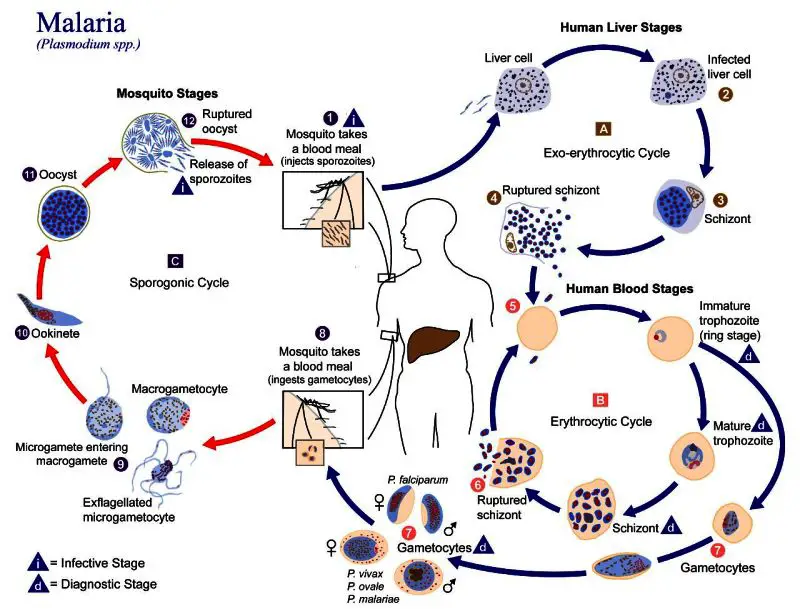
Malaria is caused by Plasmodium parasites. These are single-celled protozoans, which are not bacteria or viruses. This means that they behave differently from the germs that cause a cold or typhoid. There are a total of five species that infect humans, with Plasmodium falciparum causing the most deaths in Africa.
As Xing, Lazarev and Woo lay out in their review, the parasite lives a two-host life. It begins when an infected Anopheles mosquito bites a person and injects sporozoites, the mobile form of the parasite. Those sporozoites travel to the liver, hide inside liver cells for days, then burst out as merozoites. Merozoites are built to invade red blood cells. While inside a red blood cell, they mature through ring, trophozoite and schizont stages, then the cell ruptures and releases dozens more merozoites to infect new cells. That rupture is what triggers the classic fever spikes every 48 or 72 hours. A few parasites turn into gametocytes, the sexual form, which a mosquito picks up in its next blood meal to continue the cycle.
This biology explains why timing matters. Early symptoms such as, fever, headache, chills, body aches, look like many common infections, so clinicians cannot rely on symptoms alone. The review notes WHO data showing that when uncomplicated falciparum malaria is treated promptly with artemisinin-based combination therapy (ACT), mortality in children under five drops to about 0.07%, with a protective efficacy of 97 to 99%. Without treatment, that same group faces roughly 5% mortality under age two, and 2% for ages two to five. In severe malaria cases, even with hospital care, fatality ranges from 10% to 50%, with cerebral malaria killing about 19% of hospitalized children.
The tools we have relied on for 140 years
If you walk into most clinics in Nigeria today, diagnosis still depends on methods used before your grandparents were born. Xing, Lazarev and Woo devote a full section of their review to these traditional tools, grouping them the way lab manuals do, because each one solves a different piece of the puzzle.
Microscopy
Light microscopy is called the gold standard, as it is the oldest method for diagnosing malaria. You take blood, make two slides, stain with Giemsa, Wright’s or Field’s stain, then look for parasites inside red cells.
- A thick smear concentrates blood so you can spot parasites quickly.
- A thin smear spreads cells out so you can see shape and name the species.
It works, but only if conditions are right. On average, a microscopist usually needs more than 100 infected cells per microliter to see anything. They must scan at least 200 fields before calling a slide negative, which is slow. The authors list the core limits plainly: "laborious to prepare and thereby unsuitable for use in a high-throughput setting" and "the necessity for microscopic expertise makes this method less effective in areas in which malaria and such expertise are rare". Accuracy also drops with low parasitemia or mixed infections.
Fluorescence microscopy adds a dye that lights up parasite DNA, but sensitivity still falls fast at low levels.
Clinics piloting phone-based AI often start with a USB digital microscope that clips to a smartphone.
Hemozoin detectors and lab machines
Malaria parasites leave behind hemozoin, a crystal-like waste product. Mass spectrometry can find it in under a minute with tiny blood volumes. The downside is that the equipments are expensive and it cannot distinguish P. falciparum from P. vivax.
Rapid diagnostic tests (RDTs)
RDTs are the dipsticks most community health workers carry. Blood flows across a strip coated with antibodies that catch parasite proteins. Results come in 15 to 30 minutes, tools are cheap, and they can separate falciparum from non-falciparum.
The review is clear about the trade-offs:
- They miss low-density infections and struggle with P. ovale and P. malariae
- Some strains have deleted the pfHRP2/3 gene RDTs target, so the test fails even when parasites are present
- They give a yes/no answer, the review states that "they also do not indicate the level of parasitemia"
DNA methods: PCR, LAMP and microarrays
When you need certainty, you amplify DNA. PCR is "considered the most accurate diagnostic method" and is 20 to 50 times more sensitive than microscopy. It identifies species, catches mixed infections, and can flag drug-resistance markers. The downsides include the following
- thermocyclers cost money,
- runs take hours, and
- power is not guaranteed.
LAMP works at constant temperature so you skip the thermocycler, but you still need cold-chain reagents and specialized instruments. Microarrays are 10 to 100 times more sensitive than light microscopy and need only 15 minutes to read, yet the fluorescent detector is expensive and needs stable electricity.
Antibody tests
Serology does not find the parasite, it finds the immune response. The review notes these tests "work by detecting the antibodies that an individual develops" and can pick up infection before symptoms or smears turn positive. The problem is timing, because in acute illness antibodies may not exist yet, and a positive result could mean an old infection. ELISA improves sensitivity by detecting antigens directly, but it still needs lab equipment and time.
The role of AI
None of these tools are bad. Each was a breakthrough in its era. Together they show the same pattern: high accuracy usually means high cost, training, and infrastructure. Speed usually means loss of detail. That is exactly the gap the review says AI is trying to fill, not by inventing a new chemical, but by making the interpretation step faster, cheaper, and less dependent on scarce experts.
| Decade | Diagnostic | Development Impact / Limitations |
|---|---|---|
| 1880s | Microscopy – Discovery of Plasmodium parasites by Alphonse Laveran | First visualization; foundation for malaria diagnosis; limited by skill and sensitivity. |
| 1890s | Improved staining (Romanowsky, Giemsa) | Enhanced visualization; required trained microscopists. |
| 1900s–1940s | Standardized microscopy | Established as the gold standard; reproducibility issues. |
| 1950s | Thick and thin blood smears | Improved detection and species differentiation; labor intensive. |
| 1960s | Microscopy + clinical diagnosis | Symptom-based screening in low resource settings; nonspecific, frequent misdiagnosis. |
| 1970s | Quantitative blood smears | Parasite density estimates enabled treatment monitoring; still time consuming. |
| 1980s | Monoclonal antibody research for antigen detection | Proof-of-concept for immunoassays; not widely deployed. |
| 1990s | Rapid Diagnostic Tests (RDTs) | First true point-of-care tests; limited sensitivity for non-falciparum species. |
| 2000s | Wider adoption of RDTs | Increased accessibility in rural areas; variability in accuracy and stability. |
| 2010s | Molecular methods (PCR) | High sensitivity and specificity; costly, infrastructure heavy. |
| 2020s | Advanced molecular assays (LAMP, multiplex PCR) | Surveillance and detection of lowdensity infections; moderate cost; not fully field-deployable. |
| 2020s–present | AI-powered diagnostics Deep learning for automated microscopy, smartphone-integrated tools, AI-enhanced image analysis, microfluidics, and multi-omics integration. | Improved sensitivity and standardization; reduced inter-observer variability; potential for real-time surveillance. Challenges include data quality, cost, and generalizability |
The table above outlines the historical timeline of malaria diagnostic method development, progressing from microscopy to antigen-based and molecular approaches, and most recently to AI-powered diagnostics
How AI learned to see malaria
Xing, Lazarev and Woo show AI as a steady climb from hand-tuned rules to networks that teach themselves what a parasite looks like.
From handcrafted features to self-learning
Early machine-learning work relied on people to pick features, size, color, texture, then feed them to classifiers like support vector machines. The review notes those methods "often had difficulty with generalizability, as performance was highly dependent on the selected features". That bottleneck pushed researchers toward deep learning.
CNNs changed the game in the mid-2010s
Convolutional neural networks, CNNs, do not need a human to define a parasite. They learn hierarchical patterns directly from raw blood-smear images, from simple edges to complex parasite shapes .
You can watch and learn how this happens step-by-step in a free interactive CNN tutorial on Scrimba .
The authors write that CNNs "revolutionize not only various computer vision tasks generally but also malaria diagnostics specifically", and early implementations "outperformed earlier ML-based methods".
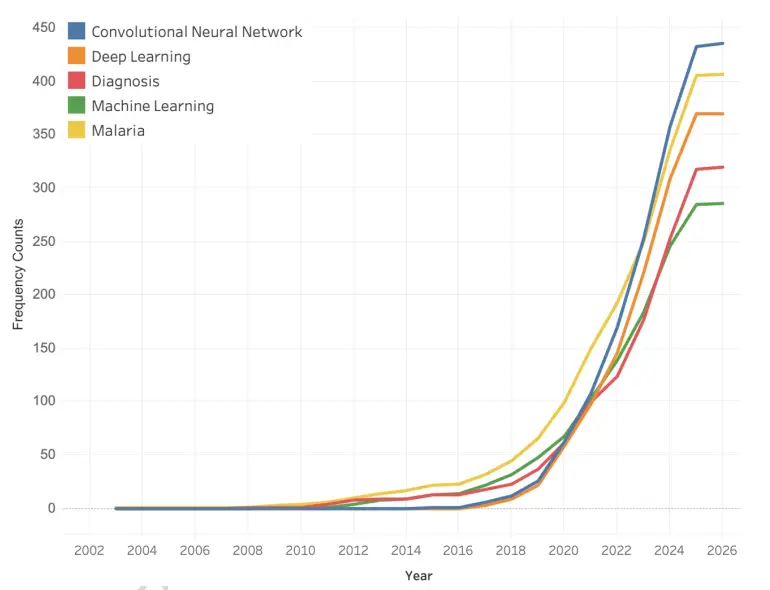
Annual frequency of AI-related keywords in malaria research publications. The figure shows increased interest in AI applications for malaria.
Performance in controlled studies quickly climbed:
- A custom CNN reported about 97% accuracy on the NIH malaria cell dataset
- A VGG-based ensemble reached about 97% accuracy, a residual-learning model about 98% accuracy
- Hybrid ensembles that combine several CNNs have pushed even higher, with one reporting 99.5% accuracy and 99.9% AUC under patient-level cross-validation
These numbers come from lab-curated image sets, not busy clinics, which the authors stress throughout.
Transformers look at the whole picture
Unlike CNNs that scan local patches, Vision Transformers use self-attention to capture long-range relationships across an entire smear. That helps with messy real-world slides where staining varies. Sengar et al. used a ViT to classify P. vivax life stages at 90.03% accuracy, and Tan and Liang reported up to 99.9% accuracy with transformer models plus synthetic data augmentation.
Pluralsight's Vision Transformer path covers the exact architecture and data-augmentation pipeline.
Multimodal systems bring context
Next-generation tools do not stop at images. These systems increasingly adopt multi-modal AI approaches, integrating data from diverse sources such as microscopy images, RDT results , genomic data, and clinical records . One example combined a smartphone RDT reader with clinical decision support to standardize field interpretation. This is important in Africa, especially in places like Nigeria, where fever could be malaria, typhoid or dengue, and context improves the diagnosis.
Speed and scale, where AI really separates
Manual microscopy takes about 20 to 60 minutes per sample. According to other reports , AI platforms scan more than 200,000 red blood cells within 7 to 10 minutes, with diagnostic accuracy comparable to, or even exceeding, expert microscopists. This is roughly 100 times the WHO recommended manual count of 500 to 2,000 cells. That throughput is why the authors say AI can improve reproducibility and reduce reader variability, not just match accuracy.
From papers to products
The review moves from lab benchmarks to commercial systems already in trials:
- Noul’s miLab MAL automates smear prep, imaging and analysis at the point of care. In a U.S. reference lab it showed 100% sensitivity and specificity, and in Ethiopia and Ghana it outperformed routine microscopy, achieving 97.4% sensitivity in low-density infections.
- Systems like miLab and AIDMAN typically report sensitivities of 88 to 95% and specificities of 93 to 98% in standardized testing, though performance drops at very low parasitemia.
Noul’s miLab MAL represents an integrated AI-powered platform that automates blood smear preparation, imaging, and analysis for point-of-care malaria diagnosis
The authors are skeptical because these tools still need large, diverse training sets and stable power or offline capability to work in rural clinics.
What AI actually changes on the forefront
The paper is careful not to confuse a high accuracy score on a clean dataset with a reliable test in a busy clinic. Xing, Lazarev and Woo spend several pages comparing speed, cost and robustness, because those are the numbers that decide whether a mother in a rural area waits minutes or hours.
Speed is not just convenience
Manual microscopy takes about 20 to 60 minutes per sample, and that assumes a trained personnel is available. Automated systems routinely examine 100,000 to 200,000 cells, compared with the WHO manual recommendation of about 500 to 2,000 cells. That 50 to 100-fold difference matters most for low-density infections, the cases RDTs often miss.
Accuracy in the real world, not just the lab
In standardized testing, systems like Noul’s miLab MAL and AIDMAN typically show sensitivities of 88 to 95% and specificities of 93 to 98%, with performance dipping at very low parasitemia. The paper reports that miLab specifically has moved beyond bench tests:
- It automates smear preparation, imaging and analysis at the point of care
- In a U.S. reference lab it reached 100% sensitivity and specificity for low-density infections, higher than conventional microscopy
- In a multicenter study of 2,201 febrile patients in Ethiopia and Ghana, miLab achieved 97.4% sensitivity, outperforming routine health-center microscopy
That Ethiopia-Ghana data is the kind the authors want more of: same disease, different labs, different slide quality, and with real patients.
Cost looks different over time
Traditional tools have hidden costs. Microscopy is cheap for slides and stains, but "long-term expenses rise due to the need for skilled personnel, ongoing training, and quality assurance". PCR gives high sensitivity but needs thermocyclers, reagents and stable power, making routine use financially challenging in resource-limited areas. RDTs are affordable per test, but mass campaigns add up and supply chains break.
AI flips the script. With "significant initial investment in data collection, algorithm development, and system validation", plus maintenance and updates, automation can lower per-test cost in high-volume settings because you need less expert oversight and you can scale across clinics. That trade-off only works if the model was trained on data that looks like your patients.
The equity bottleneck the paper keeps returning to
Model reliability depends on "large, high-quality, and geographically diverse datasets to ensure generalization across populations". The authors also flag infrastructure issues such as "unstable internet connectivity in rural settings, which can limit deployment of cloud-based AI platforms". In practice that means that for African countries with high cases of Malaria fatalities such as Nigeria:
- A model trained only on Asian or North American slides will likely underperform on local P. falciparum strains and local staining practices
- Tools that can run offline, or on a phone with a small microscope attachment, are far more useful than cloud-only systems
The review does not claim AI solves workforce shortages. It argues AI can make one trained technician supervise ten sites instead of one, by removing the most variable step which is "human readers undergoing fatigue".
What is still missing?
For all the promising accuracy numbers, Xing, Lazarev and Woo are blunt in their final sections: most AI models have never been tested where malaria actually live, and the field still lacks the basics that would make them trustworthy.
The authors list five gaps that keep coming up in the literature.
1. Annotation standards are all over the place
"First, inconsistencies in annotation standards remain a major challenge". Different labs label parasites differently, use different stain protocols, and rarely share the exact criteria for what counts as positive. Without shared guidelines curated by expert microscopists, models learn dataset quirks instead of biology.
2. Datasets are too small and too narrow
Many foundational studies lean on the NIH Cell Images for Malaria Detection set, roughly 27,000 to 27,558 labeled red blood cells. That sounds large until you realize it covers mostly one species, one strain, and one camera type. The review notes newer efforts sometimes use as few as 881 to 1,388 smear images, and clinical validation studies range from just 46 patients to about 2,250. Small, non-diverse data means models often fail on new slides, especially for non-falciparum species. The authors call for "diverse datasets and developing robust multi-species classification models".
3. Counting parasites, not just finding them, is still hard
The authors note that "parasite density quantification remains a significant technical limitation". Differences in slide preparation, how many red cells you count, and detection thresholds cause systematic underestimation, which matters for treatment monitoring and drug-resistance tracking.
4. Good tech does not guarantee survival in the market
Despite strong lab results, several commercial platforms have been discontinued. The authors point to "the discontinuation of commercial AI-powered malaria diagnostic platforms (e.g., Parasight, iMAGING)" as a warning sign. Sustainability needs more than accuracy, it requires regulatory approval in multiple countries, affordable pricing, supply chains for cartridges, and funding that lasts beyond pilot grants.
5. Over-reliance on microscopy
"AI applications beyond microscopy represent an underexplored opportunity". The authors argue that the future is multimodal, combining smear images with RDT photos, patient symptoms, travel history, even genomic data, to build a fuller picture, especially for low-density or mixed infections.
The paper ends with a to-do list. Standardize annotations, build open-access repositories with African slides, refine density estimation, design for offline use, and test in real clinics, not just reference labs. Until then, the authors warn, models risk "exploiting dataset artifacts rather than medically relevant features".
Conclusion
The review by Xing, Lazarev and Woo ends with a reminder that AI works best when it extends the reach of people who already know what they are doing.
Across 140 years of diagnostics, each tool traded one strength for another. Microscopy gave detail but needed experts. RDTs gave speed but lost counts. PCR gave certainty but needed labs. AI, especially CNNs and newer transformers, offers something different: the consistency of a machine that can scan 200,000 cells in minutes, without fatigue, and the scalability to run on a phone or a small benchtop device in a clinic with no microscopist on duty.
That promise only holds if we fix what the authors keep circling back to. Models need diverse, well-annotated local datasets, that is specific to the regions where they are applied, not just curated NIH images. The models need validation "in real-world conditions and healthcare infrastructure integration to fully take advantage of AI's consistency, scalability, and accessibility".
For researchers, the call is to share data and test in endemic settings. For policymakers and stakeholders across sub-Saharan Africa and around the world, the call is to treat AI diagnostics like essential infrastructure, not a one-off gadget. Fund local validation, set annotation standards, and require real-world performance before scale-up.
Read the full paper here: A scoping review of traditional and artificial intelligence methods in malaria diagnostics